News and Award
About CMUH
EKOS Assisted Thrombolysis:A New Weapon to Open Occluded Vessel
Chief, Section of Peripheral Vascular Disease, Division of Cardiology,
Department of Internal Medicine, China Medical University Hospital
Section of Peripheral Vessels, Division of Cardiology /
Director Chung-Ho Hsu, M.D.
A 27-year-old pregnant woman for 11 weeks suffered from chest pain, dyspnea, and syncope hence was referred to our center for further treatment. At our emergency room, saturation was 95% on nasal cannula with Oxygen 3 liter per minute, blood pressure was 96/68 mmHg, and heart rate was 123 beats per minute. Chest CT scan disclosed bilateral massive thrombus over pulmonary trunk (Figure 1), and echocardiography disclosed pulmonary hypertension (44 mmHg) with right ventricular dilatation (Figure 2). We set two EKOS catheters into bilateral pulmonary trunk emergently for pharmaco-mechanical thrombolysis (Figure 3). Thrombus over bilateral pulmonary trunk disappeared 18 hours later (Figure 4), and pulmonary pressure decreased to 23 mmHg.
We also found massive thrombus over left iliac vein and femoral vein. We set another EKOS catheter into her left leg vein to perform pharmaco-mechanical thrombolysis and thrombus was removed successfully 2 days later. She discharged one week later with regular outpatient clinic follow up under regular enoxaparin injection. She delivered 8 months later with a healthy baby and she also performed well with good recovery of exercise ability.
This young lady suffered from life threatening pulmonary embolism due to left leg severe deep vein thrombus. She was pregnant for 11 weeks already. Treatment choice included intravenous thrombolytic agent, pharmaco- mechanical thrombolysis with EKOS, and surgical embolectomy. There will have higher mortality, also high chance of abortion after surgical thrombectomy. For intravenous thrombolysis, there will be less effective, also with risk of intra-cranial hemorrhage and abortion.
The new generation therapy, so called EKOS directed thrombolysis, utilize EKOS catheter to deliver thrombolytic drugs into pulmonary artery and use ultrasound energy to vibrate the thrombus to facilitate thrombolysis. The thrombus clearance rate is over 90 percent, and the total thrombolytic agents dose is about one in fifth compared with intra-venous thrombolysis, which explained why there is low chance for intra-cranial hemorrhage. This kind of therapy also have the advantage that it affects little to the fetus. EKOS directed thrombolysis is an effecticve and safer treatment modality.
Now we already have more than 160 experiences of EKOS directed thrombolysis and our center is the biggest and also the first EKOS center in Asia. We also organize a 24-hour-operating thrombolysis team to fight the thrombus, hence we can treat the patient who suffered from thrombus related problem immediately without delay for anytime of the year.
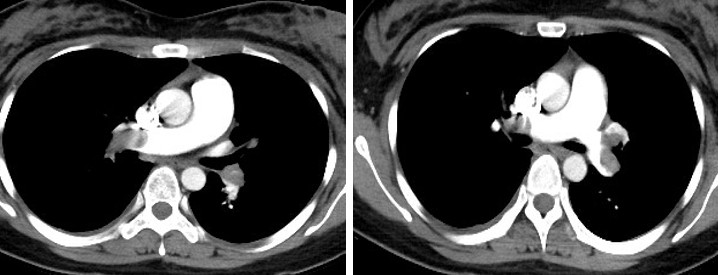
▲(Figure 1) Chest CT disclosed massive thrombus over bilateral pulmonary artery
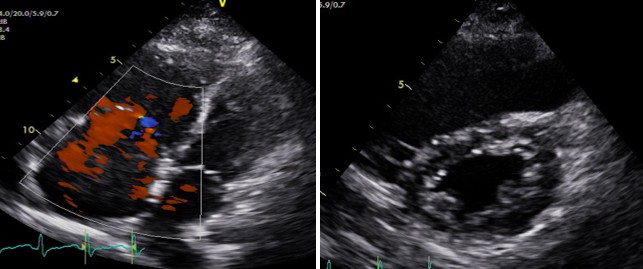
▲(Figure 2) Echocardiography disclosed pulmonary hypertension with right ventricular dilatation
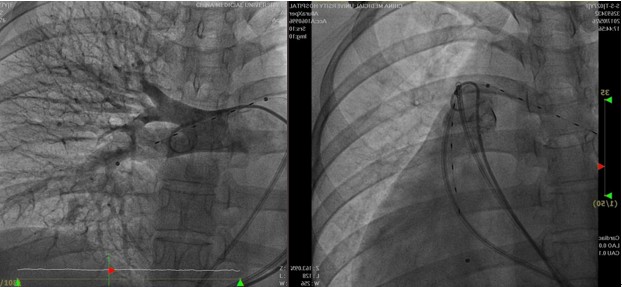

▲(Figure 3) Upper panel: pulmonary angiography disclosed two EKOS catheter in bilateral pulmonary arteries. Lower left panel: EKOS machine. Lower right panel: cartoon picture to demonstrate who EKOS deliver ultrasound energy to shock the thrombus
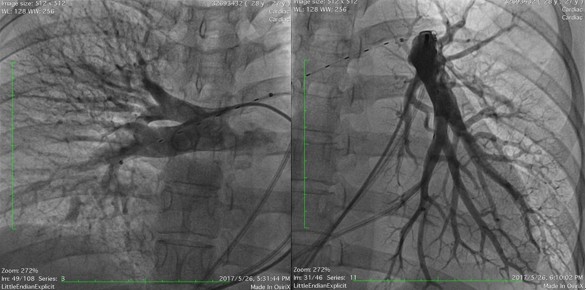
▲(Figure 4) Pulmonary angiography showed patent bilateral pulmonary arteries without residual thrombus

▲(Figure 5) 24-hour-operating acute thrombolysis team


